
False tug-back? False tug-back is the opposite of true tug-back!
When trying in a master cone, prior to obturating, we have always been told to make sure you have good “tug-back”. What exactly is good tug-back? And Why?
Well, having true tug back ensures:
- There is a better apical seal
- Canal preparation matches master point closely
- Obturation is more likely to be better sealing
- GP is not extruded beyond the foramen during down packing
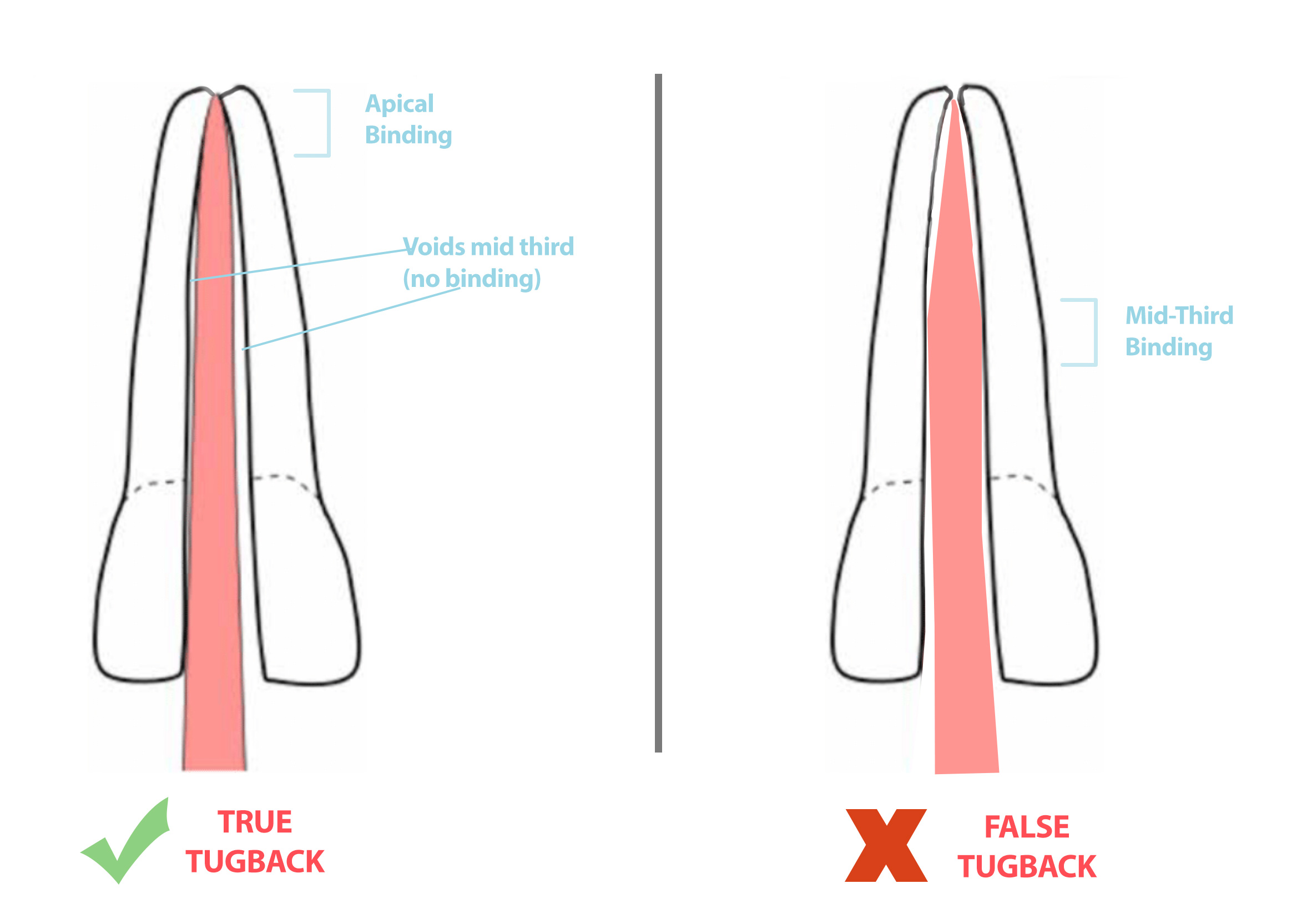 When file taper and GP taper don’t match, you get either over/under fitting GP, or GP that doesn’t bind apically. False tugback is when the master cone goes to length with apparent tugback, but is not binding apically, but rather binds more coronally or in the mid third!
When file taper and GP taper don’t match, you get either over/under fitting GP, or GP that doesn’t bind apically. False tugback is when the master cone goes to length with apparent tugback, but is not binding apically, but rather binds more coronally or in the mid third!
If you have false tugback, you are not sealing the canal apically with GP and potentially allowing an ingress of bacteria into the canal space! Additionally, if you try to obturate a canal with warm vertical condensation and have not got true tug back, then you risk extruding GP!
How to check for true tug back
- Make sure your canals are prepared and clean. Always check your master cone with a wet canal assuming canals would have sealer in the final obturation. (prior to obturation, the canals have to be dry though!)
- Do some apical gauging to help you choose your master cone.
- Insert the cone into the canal gently and check that it lightly binds.
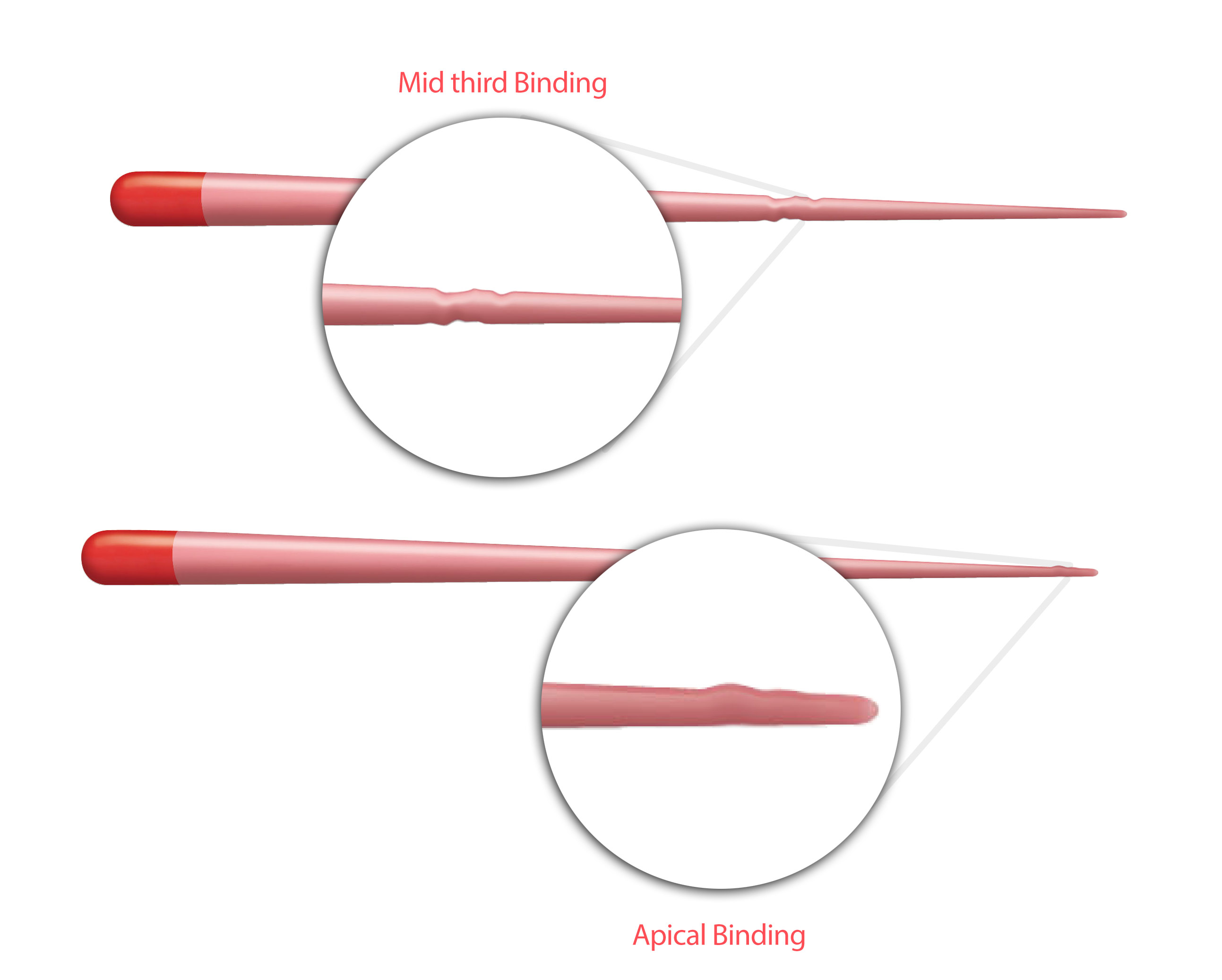
- Remove the cone and inspect it (ideally under magnification) to check for GP crimping or surface marks to indicate where the GP has been binding. Any crimping marks should be apically and not coronally! If you see mid or coronal crimping or marks, then more coronal/mid third flaring of the canal is needed! (see the image below)
Another way to check for true tug back, is to check your master cone radiograph. If you see a space mid or coronal third, but no space apically around the gp cone, then you know the GP is binding apically. If you are using a fitted cone, you may not see any space around the sides.
What to do if you don’t have true tug-back?
If you know there is no mid third or coronal binding of GP, but still have no tug back apically, then consider trimming 0.5mm from the end of your master cone and recheck. You could also enlarge your preparation using some hand K files and try a larger master cone.
If it is still difficult to get any tugback, then consider using Auto-fit GP cones which can be trimmed to length. Ideally you would use these for warm vertical condensation obturation.
If you have false tug-back (i.e tug-back but GP not binding apically), then increase the taper of the canal with more coronal and mid third flaring – applying brushing movements with the rotary file away from the centre of the tooth.
Image 1 adapted and modified from “modern endodontic principles” @Researchgate
Feature Image by UdayEndo
Thank you for your valuable information,which is more important step in the root canal treatment and which favours the success of the root canal therapy
Endodontic disease is caused by bacteria. So the most important aim is to get rid of bacteria within the tooth. Both the biomechanical prep and the chemical irrigation help do this. So in my opinion it using your irrigant effectively (NaOCl) that increases success rate.
Of course all steps need to be done well:)
But once u clean ur room it’s windows and rooms should be shut to close the door, else dust will come again and unclean ur rooms…
Just like that for future success obturation also an integral step u should not misscare there
Helpful information
Thanks for information
Thanks for this important & usefull knowledge .
nicely explained
Thank you
i love that info
thanks
why there is no tug back after insertion of gp?